Vidéo trouvée sur Points de Vue

Vidéo trouvée sur Points de Vue
Article trouvé sur Points de Vue Auteur : Kirk L. Smick, docteur en optométrie et membre de l’Académie américaine d’optométrie. Chef des services d’optométrie, The Clayton Eye Center, Marrow (Géorgie), aux États-Unis
La dégénérescence maculaire liée à l’âge (DMLA) et la cataracte impactent fortement
le système de santé américain. Un large effort de prévention de ces affections
fait maintenant partie des initiatives en optométrie. Dans un souci de productivité autant que d’économies pour la société, les optométristes se concentrent sur quatre domaines de pratiques préventives : la prescription de verres protecteurs, les compléments alimentaires, les tests génétiques et les contrôles visuels périodiques.
En février 2014, environ 24 optomé- tristes se sont réunis à l’Université de Houston à l’occasion de la première Ocular Surface Disease Wellness Conference. Les sujets du «bien-être» et de la «prévention» des maladies ont été abordés lors de cette conférence historique de deux jours. Avant la conférence, des rencontres plus spécialisées entre optométristes ont permis de discuter de diagnostics et de traitements de maladies, plutôt que de prévention. Le concept de prévention de maladie est unique dans le domaine de la santé visuelle. La myopie peut toutefois faire exception à cette règle, car de nombreux efforts sont déployés pour retarder sa progression à l’aide de lunettes à double-foyers, de lentilles de contact (orthokératologie) et d’agents pharma- cologiques (atropine)1. Une réunion de suivi est prévue en décembre 2014 à Dallas (Texas).
Parmi les affections qui se prêtent à des discussions de prévention par les optométristes aux États-Unis, on retrouve les pathologies oculaires de surface, les dommages oculaires dus à la lumière visible à haute énergie et les dommages causés par la lumière ultraviolette. La dégénérescence maculaire liée à l’âge (DMLA) et la cataracte jouent un rôle majeur dans le système de santé américain et tous les efforts de prévention de ces affections seront bénéfiques pour la société aussi bien en termes financiers que de productivité. À l’heure actuelle, la chirurgie de la cataracte est l’acte chirurgical le plus répandu aux États-Unis. Le coût moyen de l’opé- ration, qui s’élève aujourd’hui à 3 230 dollars par œil2, est en hausse en raison de l’utilisation de nouvelles technolo- gies (chirurgie laser et implants multifocaux). Le coût global de la défi- cience visuelle due à la dégénérescence maculaire liée à l’âge est estimé à 343 milliards de dollars3.
Dans le cadre de la prévention de la DMLA, les optométristes américains se concentrent aujourd’hui sur quatre domaines de mesures préventives : les compléments nutritionnels, les tests génétiques, les traitements de verres spécialisés pour bloquer certaines lon- gueurs d’ondes de la lumière bleue et enfin les examens périodiques du fond d’œil couplés à des études de tomographie par cohérence optique (OCT). Bien qu’il existe plusieurs modèles de tomographie par cohérence optique, nous sommes personnellement satisfaits de notre nouvel instrument CirrusTM HD-OCT. L’évaluation du risque génétique de dégénérescence maculaire liée à l’âge est de plus en plus fréquemment utilisée aux États- Unis pour les patients présentant des facteurs de risque.
Steve Arshinoff4 a écrit : «Auparavant, nous tenions compte de l’aspect phénotypique de l’œil, des niveaux de pigments maculaires et des facteurs non génétiques liés au patient pour déterminer le risque de DMLA»4. Le génotypage qu’il est possible de réaliser grâce aux tests génétiques disponibles dans le commerce (Macula RiskTM, RetnaGeneTM) nous permet désormais de prédire avec un degré de précision de 90% le risque de progression vers une DMLA avancée sur des périodes de deux, cinq et dix ans. Suite à la publication des résultats de la deuxième étude sur la dégénérescence maculaire liée à l’âge (AREDS2), nous disposons à présent d’informations définitives sur la prévention et la progression de la DMLA à l’aide notamment de compléments nutritionnels, même si de nouvelles recherches sont nécessaires.
Le nombre de personnes vivant avec une dégénérescence maculaire est similaire au nombre de personnes atteintes d’un cancer invasif, quel qu’il soit5. Aux États-Unis, onze millions de personnes sont atteintes d’une forme de dégénérescence maculaire liée à l’âge. Un chiffre qui devrait doubler d’ici 2050. La plupart des chercheurs estiment que l’exposition à la lumière bleue joue un rôle dans la pathogenèse de la DMLA. Selon Margrain et al.6 : «Les signes biochimiques ont démontré que des réactions photochimiques dans l’environnement riche en oxygène de la rétine externe conduisent à la libération de dérivés actifs de l’oxygène (DAO) avec des effets cytotoxiques. Ces DAO provoquent un stress oxyda- tif, qui est connu pour contribuer au développement de la DMLA. Le chromophore précis qui peut être impliqué dans la pathogenèse de la DMLA est mal connu mais la lipofuscine (pigment du vieillissement) est un candidat probable». Et de poursuivre : «Les études sur la densité des pigments maculaires humains et le risque de progression de la DMLA après une chirurgie de la cataracte donnent encore plus de poids à l’hypothèse selon laquelle l’exposition à la lumière bleue joue un rôle dans la pathogenèse de la DMLA mais les signes épidémiologiques sont équivoques. La lumière bleu- violet a un double effet sur la lipofuscine. Elle provoque une augmentation de la production et active également ses composantes phototoxiques (radicaux libres), provoquant la mort des cellules de l’épithélium pigmentaire rétinien. Dans l’ensemble, les signes suggèrent, sans toutefois le confirmer, que la lumière bleue est un facteur de risque dans la DMLA.»7 Les recherches menées par le Schepens Eye Institute (Université de Harvard) suggèrent qu’une faible densité de pigment maculaire peut également représenter un facteur de risque de DMLA puisqu’elle permet à la lumière bleue de causer plus de dommages.

Présentation de verres Crizal®Prevencia® à une patiente
À l’heure actuelle, il existe fondamentalement deux sources de lumière artificielle : à incandescence (dont les halogènes) et luminescente (fluo- rescentes et LED). Les ampoules à incandescence sont de plus en plus difficiles à trouver dans les magasins de bricolage aux États-Unis, car les nouvelles sources de lumière à LED commencent à les remplacer. Ces nouvelles sources de lumière, beau- coup plus économes en énergie, ont une durée de vie supérieure et le gouvernement américain a décrété que la transition était en cours. On pense que d’ici 2020, 90% des sources de lumière dans le monde seront basées sur des LED et des produits d’éclairage à l’état solide. Ces sources de lumière plus récentes dégagent plus de lumière bleue que les anciennes ampoules à incandescence. Nous savons que le soleil est la source de lumière standard. La proportion de lumière bleue dans la lumière du jour, dans l’ensemble du spectre visible, oscille entre 25% et 30%. Nous savons que la lumière bleue est vitale pour un certain nombre de processus physiologiques et qu’il pourrait se révéler mauvais d’interférer dans ce processus8. Une étude récente menée par Gray et al dans le Journal of Cataract and Refractive Surgery révèle que les
patients possédant des implants intraoculaires multifocales filtrant la lumière bleue présentent des résultats nettement meilleurs dans des conditions de conduite avec éblouissement que des patients semblables possédant des lentilles intraoculaires transparentes. Le docteur Henderson et ses collègues n’ont constaté aucun problème dû aux filtres de lumière bleue, du moins dans les paramètres visuels : ils estiment «que la protection potentielle contre la DMLA en vaut la peine»9.
Plusieurs équipes du monde entier ont étudié les risques potentiels pour la santé des produits contenant des LED. Fondamentalement, trois populations à haut risque ont été identifiées : (1) les enfants et les aphakes qui reçoivent une proportion supérieure de lumière bleue sur la rétine, (2) les personnes souffrant de pathologies photosensibles oculaires ou utilisant des médicaments photosensibles (agents sensibles à la lumière employés en thérapie photodynamique comme la Vertéporfine utilisée pour l’ablation des vaisseaux sanguins dans l’œil lors du traitement de la dégénérescence maculaire humide) et (3) les personnes quotidiennement exposées à des LED à de courtes distances de la source.
En pratique, les optométristes et les ophtalmologistes aux États-Unis ont commencé le processus d’utilisation des dossiers médicaux électroniques (ObamaCare). Pendant la première partie de l’examen, le professionnel pose plusieurs questions au patient. Puis, s’il entre dans l’un des trois groupes ci-dessus, le professionnel le conseille sur les risques particuliers auxquels il fait face et lui prescrit des verres qui l’aideront à se protéger des
menaces dues à une présence accrue de lumière bleue. Dans la mesure où nous sommes les gardiens d’une bonne vue, il est important pour nous, optométristes, de conseiller les patients sur les facteurs de risques modifiables. Deux de ces facteurs de risques sont le tabagisme et l’exposition chronique à la lumière, notamment aux UV et à la lumière bleue
(lumière visible haute énergie). Nous avons compris au Clayton Eye Center de Morrow, en Géorgie, que l’on obtient de bien meilleurs résultats lorsque le professionnel lance lui-même la conversation sur la protection contre la lumière bleue en salle d’examen et que l’opticien renforce ensuite le message. Nous prescrivons spécifiquement le nouveau traitement de verre Crizal® Prevencia® afin de filtrer de manière sélective uniquement les longueurs d’ondes dangereuses, tout en laissant passer les bonnes longueurs d’ondes. Nous savons que les lon- gueurs d’ondes bleues constituent la partie la plus puissante du spectre électromagnétique visible pour la régulation du rythme circadien. Comme la durée et la quantité de lumière et d’obscurité ont toutes deux une incidence sur le sommeil, l’utilisation en soirée de verres de couleur orange pour bloquer la lumière bleue pourrait améliorer la qualité du sommeil. Nous avons compris au cours des derniers mois que nos patients apprécient le fait que nous protégions leurs yeux en en discutant avec eux et nous pensons qu’il serait vraiment dommage de ne pas les informer. Nous faisons référence aux données des études Beaver Dam et Blue Mountain qui démontrent que la lumière bleue est un facteur de dégénérescence maculaire liée à l’âge, notamment après une chirurgie de la cataracte. Notre clinique effectue plus de 3 000 chirurgies de la cataracte par an et chaque visite post-op souligne le risque potentiel que représente la lumière bleue. Nos implants intraoculaires sont équipés d’un filtre contre la lumière bleue pour assurer une protect
on supplémentaire. Notre cabinet participe depuis peu à un programme accéléré mettant l’accent sur la délivrance dirigée par les médecins. Nos neuf optométristes prescrivent à présent divers produits et verres préventifs à chaque patient lorsque cela est indiqué, présentent les produits concernés sur un formulaire spécialement conçu à cet effet et les examinent avec le patient. Le patient est ensuite escorté vers le département optique de la zone clinique par un technicien ou le médecin et le formulaire est présenté à l’opticien. Les produits tels que les traitements antireflet, Transitions®, les verres progressifs réalisés par surfaçage numérique (tels que le Varilux® S SeriesTM) et les traitements Crizal® Prevencia® ont considérablemen augmenté grâce à ce nouveau processus.
Plusieurs fabricants de verres se sont engagés dans la technologie de blocage de la lumière bleue. Mais jusqu’à présent, seul Essilor a conçu un traitement qui bloque des lon- gueurs d’ondes spécifiques. Les verres Unity BlueTech de VSP, RechargeTM de Hoya, iBlucoatTM de PFO et BlueTech de Signet Armorlite (intérieurs et extérieurs) bloquent tous la lumière visible haute énergie et offrent une meilleure sensibilité aux contrastes. En revanche, ils bloquent aussi la plage de lumière bleu-turquoise, qui est une «bonne» lumière nécessaire pour d’autres fonctions, y compris pour améliorer la sensibilité aux contrastes et réguler la bonne humeur.
La deuxième étude AREDS2 était un essai multicentrique aléatoire visant à évaluer les effets d’un apport par voie orale de xanthophylles maculaires (lutéine et zéaxanthine) et/ou d’omégas 3 à longue chaîne (acide docosahexaénoïque) et d’acide eicosapentaénoïque (AEP) sur la progression de la dégénérescence maculaire liée à l’âge (DMLA) avancée. Même si les résultats de l’étude n’ont pas permis de répondre à certaines questions, ils ont toutefois ouvert la voie à des changements en matière de prescription de complé- ments nutritionnels pour les patients atteints de dégénérescence maculaire précoce et les personnes à risque. Aujourd’hui, les optométristes américains encouragent systématiquement leurs patients à prendre ces compléments nutraceutiques dans le cadre d’une procédure et je pense que cette pratique deviendra la norme de soins d’ici peu. Plusieurs produits sont disponibles sur le marché, mais les gels Preservision Eye Vitamin AREDS 2 Formula Soft Gels de Bausch & Lomb sont probablement les plus fréquem- ment utilisés. Ce produit particulier ne contient pas de bêta-carotène, point positif pour les fumeurs et les anciens fumeurs. J’ai souvent utilisé le Macula Protect Complete de Science Based Health, lui aussi sans bêta-carotène. L’étude a démontré une réduction globale de 25% du risque de progression de la DMLA exsudative. Le rôle du pigment maculaire (PM) est également reconnu et de nombreux optométristes mesurent à présent les pigments maculaires et dosent les compléments en conséquence. Le régime alimentaire américain est connu comme étant faible en lutéine et zéaxanthine10. Le troisième caroténoïde, la méso-zéaxanthine, est un caroténoïde clé dans la macula, encore moins présent dans le régime alimentaire américain. Nous savons que les fumeurs sont très exposés à un risque de DMLA11. Chez les fumeurs et les anciens fumeurs, le bêta-carotène a été associé à un risque accru de cancer du poumon12, 13, 14.
Les tests génétiques ont progressé dans plusieurs domaines de la médecine au cours des dix dernières années. La DMLA a notamment bénéficié des avantages des recherches continues. À l’heure actuelle, nous sommes capables de pronostiquer avec un degré de précision de 90% la façon dont la maladie oculaire d’un patient va progresser15. Plusieurs projets de recherche ont démontré que les patients soumis à des tests ont de meilleurs résultats que les autres. À l’occasion de la réunion annuelle 2013 de l’American Society of Retina Specialists, le docteur Peter Sonkin, spécialiste de la rétine chez Tennessee Retina, a présenté les résultats d’une analyse de l’impact des tests génétiques menés dans leur cabinet sur une période de cinq ans. Il en ressort que les patients ayant subi des tests de risques de macula et fait l’objet d’un programme de surveillance stratifiée et d’un pro- gramme d’information des patients, avaient une meilleure acuité visuelle que les patients n’ayant pas fait l’objet de tests génétiques. Un article intitulé «Prediction of Age-Related Macular Degeneration in the General Population – The Three Continent AMD Consortium» (Prévision de la dégénérescence maculaire liée à l’âge dans la population – Consortium des trois continents sur la DMLA), et paru dans le numéro de novembre 2013 du magazine Ophtalmology, présente une évaluation des pronostics de DMLA à l’aide de trois études pros- pectives basées sur la population : la Rotterdam Study, la Beaver Dam Eye Study et la Blue Mountain Eye Study. Le modèle non-génétique présentant un statut âge + sexe + IMC + tabagisme + DMLA affiche une exactitude prédictive de 78%, tandis que le modèle génétique, reposant sur la génétique avec les critères ci-dessus, affiche une exactitude prédictive de 82%. J’ai réuni toutes les informations disponibles dans une formule résumant ce que les optométristes de soins primaires devraient faire aujourd’hui pour prévenir la perte.
En résumé, les cas de la DMLA sont en hausse. Comme les individus continuent à vivre plus longtemps, les optométristes en diagnostiqueront de plus en plus. La prévention doit être appliquée et nous disposons à présent de plusieurs outils qui nous aident dans nos efforts. Les changements d’éclairage demandés par le gouvernement nous exposeront à des doses plus élevées de lumière bleue (lumière visible haute énergie) potentiellement nocive. L’utilisation d’ordinateurs ne cesse d’augmenter et ces outils, de même que les tablettes électroniques, smartphones et autres écrans utilisés à très courtes distances, augmentent également notre exposition. En prescrivant des verres permettant de filtrer les longueurs d’ondes nocives, nous pouvons éviter à de nombreuses personnes de souffrir de cette terrible maladie. En ajoutant des tests génétiques et des compléments nutraceutiques à notre arsenal, nous pourrions rendre un grand service au monde. Notre métier est de préserver la santé visuelle et cela peut nous aider à y parvenir. Le fait de privilégier une approche «passive» consistant à attendre pour voir ce qui se passera plutôt que de mettre en œuvre le protocole ci-des- sus, peut faire plus de mal que de bien à vos patients. The Optometric Oath (serment) promu par l’American Optometric Association comprend les dispositions suivantes : «Je VAIS pro- diguer des conseils honnêtes et complets à mes patients sur tout ce qui peut servir à rétablir, conserver ou améliorer leur acuité visuelle et leur bonne santé en général. Je VAIS en permanence m’efforcer d’élargir mes connaissances et compétences pour offrir à mes patients des moyens effi- caces et inédits pour mieux prendre soin de leur vue.»
L’approche ci-dessus correspond bien à ma responsabilité.
• En 2020, 90% de toutes les sources d’éclairage dans le monde seront basés sur des LED.
• La proportion de lumière bleue dans la lumière du jour, dans l’ensemble du spectre visible, oscille entre 25% et 30%.
• Le protocole du Clayton Eye Center pour la DMLA est un recueil des bonnes pratiques et recommande les étapes suivantes :
1. Diagnostiquer la DMLA
2. Effectuer des tests génétiques sur chaque patient atteint de DMLA
3. Augmenter la fréquence de surveillance, y compris des tests de tomographie par cohérence optique (OCT)
4. Prescrire les bons nutraceutiques
5. Prescrire des verres dotés de filtres sélectifs bloquant la lumière bleue
6. Prodiguer des conseils aux patients en termes d’alimentation, de tabagisme, d’exercice et de poids (IMC) d’acuité visuelle. Ce protocole est utilisé par nos médecins et bien d’autres. Il s’agit d’un recueil des bonnes pratiques actuelles.
Article trouvé sur Points de Vue Auteur : Kirk L. Smick, docteur en optométrie et membre de l’Académie américaine d’optométrie. Chef des services d’optométrie, The Clayton Eye Center, Marrow (Géorgie), aux États-Unis
Article trouvé sur Points de Vue
Les nouvelles technologies et l’usage des supports numériques changent indéniablement les comportements posturo-moteurs des utilisateurs. Pour autant, il existe encore peu de données sur la caractérisation scientifique de ces nouvelles habitudes posturales. Récemment, les équipes de la R&D d’Essilor International ont mis au point un dispositif d’expérimentation spécifique qui a délivré des résultats originaux.
L’analyse des données posturales, mesurées dans ce cadre, a permis d’établir un cahier des charges pour la conception d’une nouvelle catégorie de verres ophtalmiques.

Article trouvé sur Points de Vue
Article trouvé sur : www.pointsdevue.com
Light-induced ocular damage has been investigated for decades in laboratory extensive work and several epidemiological studies. More recently, harmful effects of blue-violet light have been spotlighted by growing body of scientific research. Despite the eye’s natural defense mechanisms, it has been evidenced that cumulative exposure to blue-violet light can contribute to long-term irreversible changes in the retina. When the most critical exposure occurs in outdoor conditions, Transitions® lenses can effectively filter harmful blue-violet light and consequently provide optimal photo-protection for the patient eyes.
Light is an element of life, a major environmental factor in human development. It plays a significant role in how we process sensory information, impacting our visual experience from the point of birth and throughout our lives.
Visual perception occurs when light strikes the retina of the eye. The pupil of the iris serves as the optical diaphragm of the eye affecting the path of light rays which are refracted by the cornea and the crystalline lens on their way to the retina. Numerous deprivation experiments have demonstrated that ocular growth and refraction development are regulated by visual information. Light is essential in providing this information on diurnal species by transmitting signals which are converted by the brain into visual perception. This acquisition of visual function is experienced as early as infancy and is essential to healthy development.
The iris acts as a natural optical diaphragm for expanding (dilation) or retracting (constriction) its central aperture. Depending essentially on lighting conditions and age, the diameter of the pupil ranges from 2mm to 8mm. Variations in the diameter of the pupil are caused by a movement reflex that regulates the light flux incident and, subsequently, visual performance. The visual system as a whole is sensitive over a wide range of light levels from starlight to bright sunlight but, despite the regulation of the pupil aperture, it cannot operate over the entire range simultaneously. An adaptation is required to adjust the light sensitivity of the visual system to different light levels. When the adaptation is in progress, visual performance is reduced. Once the process is complete, visual capabilities depend on the new level of light.
There are two primary lighting conditions with which the visual system has to deal: daylight (photopic) and nighttime (scotopic). Between photopic and scotopic levels is a range called mesopic, which corresponds roughly to twilight. The human eye has three types of light sensitive cells (photoreceptors) in the retina – cones, rods and ganglion cells – that process sensory information (Table 1). Cones are highly concentrated in the central area of the retina (macula) and are responsible for providing daylight sharp image resolution and color detection. Rods are largely distributed in the periphery of the retina. Having high sensitivity, they are required for scotopic vision but provide low resolution and lack of color information. The ganglion cells or ipRGCs (intrinsic photosensitive Retinal Ganglion Cells) express the melanopsin-based photopigment. These melanopsin ganglion cells are crucial for relaying light information from the retina to the brain to control circadian rhythms, pupillary light reflex, sleep and many other body functions. (Sand A. et al., 2012, Gronfier 2013).[11, 09]

Table 1. Summary of main lighting conditions (Boyce, 2001).[6]
The sun emits a tremendous amount of energy in the form of wide electromagnetic radiation. From cosmic rays to radio waves (Fig. 1), the majority of solar emissions are not visible to human photoreceptors. Only a thin portion – at wavelengths (λ) between 380nm and 780nm – provides the visible light that interacts with the eye’s photoreceptors – enabling us to see the world. When visible solar radiation reaches the Earth’s surface it is scattered throughout the atmosphere, especially in the blue-violet region corresponding to the shortest wavelengths (380-460nm) of visible light and subsequently to the highest energy.

Fig. 1: Electromagnetic radiation and the visible spectrum
Beyond the visible spectrum, sunlight emits ultraviolet radiation with wavelengths shorter than 380nm – commonly referred to as UV – and infrared radiations with wavelengths greater than 780nm. Ultraviolet radiation arriving on earth surface is divided into UVB (280-315nm) and UVA (315-380nm). At sea level, about 10 percent of radiation is UV, 50 percent is visible and 40 percent is infrared.
Exposure to the sun for an extended period of time produces erythema and affects skin pigmentation, causing burning or tanning. Both UVA and UVB penetrate the atmosphere freely and play a critical role in advancing more severe health conditions like premature skin aging (ex: wrinkles) and certain skin cancers (ex: carcinoma) which can affect the eyelids and facial skin. In a healthy adult, more than 99 percent of UV radiation is absorbed by the anterior part of the eye (eyelid, ocular surface, crystalline lens). Exposure to ultraviolet radiation is well established as a major cause of eyelid malignancies, photokeratis, climatic droplet keratopathy, pterygium and cortical cataract (Yam 2014, Behar-Cohen et al. 2014). [17, 3] There is insufficient evidence to support the proposal that Age-related Macular Degeneration (AMD) is related to UV exposure, and it is now suggested that AMD risk is probably more closely related to exposure to visible radiation, especially blue light (Yam 2014). [17]
The blue sky is evidence that blue light is present in direct sunlight. Since blue light is higher in energy than other wavelengths in the visible spectrum (Fig. 2), it scatters more throughout the atmosphere (Rayleigh scattering) and makes the sky appear blue. Blue light makes up 25-30 percent of daylight.

Fig. 2: Daylight source spectra
While blue light is emitted naturally by the sun, it can also be produced by numerous artificial light sources commonly found indoors. Light-emitting diodes (LEDs) are gaining an increased share of the domestic lighting market because of their high efficiency of luminance and low energy consumption. Widely found in digital screen technologies and displays, LEDs exhibit a high emission blue peak, centered at 430nm (Fig. 3).

Fig. 3: Artificial cool white LED source spectrum
As a part of visible light, blue light passes through the eye structure, reaching the retina. Due to its higher level of energy than the other wavelengths in the visible spectrum, it is potentially harmful to the retina. Depending on exposure conditions (light intensity, duration, periodicity) it may induce different types of reactions, including photochemical lesions (Rozanowska et al., 2009). [16]. Laboratory experiments showed that blue light is harmful (Sparrow et al., 2000)[14] and particularly it has been demonstrated that exposure to blue violet light with a maximum peak centered on 435+/- 20 nm can induce irreversible cell death in the retinal pigment epithelium (RPE), located in the external layer of the retina (Arnault et al., 2013). [1] These damages contribute to the aging process of the eye and may lead to the development of pathologies such as AMD, the major cause of blindness in the elderly in developed countries. In epidemiological studies addressing long term chronic exposure to blue light, the Beaver Dam Eye study demonstrated that there is a strong correlation between outdoor activities (sunlight exposure) and early incidence of AMD changes (Cruickshanks et al., 2001, Tomany et al., 2004). [7, 15]
Amount of blue violet light is characterized by the intensity of emitted light of varied sources (Table 2). Sunlight is by far the strongest source of blue light at least 100 times greater than artificial sources (Fig. 4).

Table 2: 420-440 nm integrated Irradiance values (w/m2) of common artificial light sources against solar diffused light (Transitions Optical internal measurements)
There is a significant difference in the level of blue light when facing into the sun (direct) and facing away from the sun (indirect). In actuality, no one looks directly at the sun since there is a natural aversion to sources of high glare. Humans often make adjustments by moving their head or their eyes or by relying on automatic reflexes like blinking, squinting and pupillary constriction. The eye can be subject to more serious effects due to multiple reflections of sunlight onto white surfaces. For example, the reflection of the sun at noon on sand or snow can reach 10 times more luminance than the blue sky (Behar-Cohen et al., 2011). [4]
The impact of blue-violet light exposure depends on the amount of total light reaching the retina: the retinal irradiance, which is characterized by the radiant flux (power) received by the retina per unit area. These values vary by the ocular media transmittance and – more importantly – by physical factors such as the eyelid position, which dictates the field of vision and the pupillary aperture, making ocular dosimetry far more complex than generally appreciated (Sliney 2001, 2005). [12, 13]More investigations need to be done, but it seems reasonable to think that the level of retinal irradiance in the 435+/- 20 nm range is more important outdoors than indoors. Wearing appropriate glasses can be worthwhile to prevent from cumulative effects of light exposure.


Fig. 4: Irradiance spectra of common artificial light sources (top) and direct and indirect sunlight (bottom). (Transitions Optical internal measurements)
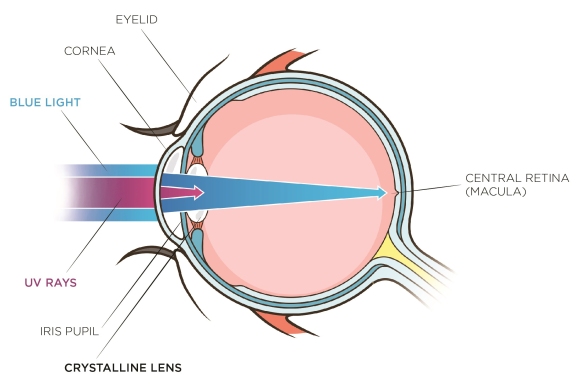
Physiological structures around the eye, like eyelids and eyelashes, provide some protection against intense light. The iris pupil also contributes by using constriction to decrease the amount of entering light. While UV transmittance is blocked primarily by the cornea and crystalline lens in healthy adults, blue light crosses over these structures to reach the fundus of the eye (Fig. 5). The amount of blue light reaching the retina depends on the age of the eye as, during a lifetime, there is a yellowing of the crystalline lens that would typically provide some absorption in the blue violet region. The central part of the retina is covered by yellow pigments (Macula Lutea), which serve as a filter for incoming blue light because its absorbance peak in this range (Haddad et all, 2006).[10] Due to assorted factors, macular pigment density can be variable from one individual to another and its ability to absorb light evolves during a lifetime. The children are the most exposed to harmful blue light because they have larger pupil diameter, less concentration of macular pigment and the amount of blue light reaching the retina is 65 % while it is 40 % for adults (Behar-Cohen et al., 2015). [5]

Fig. 5: UV and blue-violet light path into the human eye
With the potential risks associated with outdoor conditions described and the natural protections of the human eye discussed, we now turn our attention to the technical solutions available within the eyewear industry to prevent from the long-term effects of blue-violet light. UV protection in eyewear will not be reviewed here since most high-quality lenses today offer complete protection against UV up to 380nm.
Anti-reflective interferential layers may be applied to ophthalmic lenses by evaporating transparent dielectric metal oxides to the anti-scratch coating on both the convex and concave sides of the lens. The coatings essentially involve stacks created by successive deposits. Processed under vacuum on a few hundred nanometers of low index material (RI ~1.46) and high index material (RI ~ 2.2) of desired thickness (Fig. 6), they provide anti-reflective properties within the visible region of the light spectrum. It is possible to design anti-reflective stacks that offer enhanced protection in the blue-violet light region by adding a specific reflection element at the wavelength to be rejected, in this case 380-460nm. The blue-filtering reflective properties can be effective up to 20 percent while keeping superior anti-reflective properties active within the entire remaining visible range. These ophthalmic lenses display high clarity indoors and outdoors, and offer reliable indoor protection against harmful blue-violet light emitted by electronic devices and artificial lighting while providing moderate outdoor protection as well.


Fig. 6: left: Blue mirror effect of an anti-reflective coating (AR) and its reflectance spectra (right)
Another way to prevent harmful blue-violet light from entering the eye is to reduce the unwanted wavelengths by absorbing them with yellow dye, a chemical compound whose structure allows absorption in the visible part of the light spectrum of its complementary color: in this case, blue. This is why most blue-absorbing lenses appear more or less yellow depending on the level of their blue-filtering properties. A highly-efficient blue-blocking lens would appear deep yellow, while a moderately efficient blue-blocking lens would appear merely yellowish.
The advantage of the yellow dye solution is that it can reduce a significant amount of blue light, but the intense yellow color is detrimental to its cosmetic appearance and detracts from human color perception. A highly intense yellow filter, for example, will induce color distortion despite the ability of the brain to adapt chromatically.
There is a way to circumvent the yellow color of an absorbing filter that involves “color balancing” the tint by adding a small proportion of another dye. The complementary dye absorbs in another region of the visible spectrum, creating a global neutral grey filter (Fig. 7). This solution is acceptable for low yellow colors – where color balancing can be efficient – but not possible for dark yellow tones. It should be noted as well that color balancing in general is detrimental to the global photopic transmission of a lens since it causes a loss of visible transmission (or clarity).
A lens can also be surface tinted by dipping an uncoated lens substrate or a tintable coated lens in a water dye solution at an elevated temperature.
Another solution is to cast lenses with monomers that already contain yellow dyes – and its color balancing agents – in the original formulation. In this case, only light tints are achievable since darker tints would lead to a non-homogeneous appearance from center to edge due to differences in prescription lens thickness (high-minus and high-plus finished lenses).

Fig. 7: Blue light absorption with yellow dyes in substrate (left) and neutral color-balanced substrate (right)
Sunwear lenses are commonly grouped by IS0 8983-3 standards as class 3, providing 10-15% of photopic transmission (Tv), or the darker class 4 category (Tv < 8%).
In the case of prescription eyewear, sun lenses are essentially made by diffusing a mixture of dyes in a polymer substrate or in a tintable coating. For the plano sunwear business, coloring is achieved by mass mixing an injection mold of polycarbonate for instance. Polarized lenses are made by using dichroic dyes in pre-formed stretched films or encapsulated wafers. The dyes are generally a mixture of primary colors in different combinations to achieve the desired hues based on the principle of subtractive color mixing (Baillet et al., 2008). [2] The most common hues are brown and grey.
In the fashion and high-performance sunwear business, one finds mirrored lenses manufactured on the principle of interferential light rejection stacks and/or a mix of tinting by absorption and rejection mirror technologies.
By definition and usage, sun lenses are made exclusively for outdoor purposes. The dark intensity of the lenses, both plano and Rx, allows very good protection against blue light, especially by brown lenses where the yellow dye content in the mixture is in the majority (Fig. 8).

Fig. 8: Sun lenses in brown and grey showing that, at equal photopic transmission (15% Tv), the brown lens filters more blue light than the grey lens, as it contains more yellow dyes in its formulation
Photochromic lenses are non-permanent tinted filters containing photochromic dyes made from molecular structures that are reversible under the action of light (DÜrr et al., 1990). [8] Their tint or color is obtained through the same principle of color-subtractive mixing as sunwear lenses.
There are, however, several notable differences in manufacturing technologies, including the cast in place (CIP) process wherein photochromic dyes are added to the monomers before polymerization, and the imbibition process, where photochromic dyes are absorbed into the surface of a lens. In these first two examples, a dedicated polymer allows the photochromic mechanism and movements to occur, and requires different polymers for each refractive index (for prescription lenses). The coating technology, meanwhile, wherein photochromic dyes are added to a coating deposited by dip – or preferentially, by spin – allows the process to be substrate independent. Photochromic lenses are highly efficient in protecting against glare, since their darkness (photopic transmission) automatically adjusts to the amount of outdoor light, whether overcast, in shadow or in bright sunlight. Because they always acclimate to various lighting levels, they help the visual system to adapt instantaneously without compromising visual performance or comfort.
The advantage of photochromic lenses like Transitions® Signature™ lenses is that they are dark outside when sunlight is bright and intense, so they offer a high level of blue light filtering much like regular sun lenses. They can be worn all the times and offer good indoor protection against artificial blue lights with no aesthetic drawbacks such as residual yellow color (Fig. 9).
As described before, color-balancing can help to limit the yellowish aspect of a given filter. For photochromic lenses, where a very low level of yellowness needs to be overcome, the smart color balancing is put to full use. Only a slight amount of dyes are used to deceive the eye (and subsequently the brain) to offset the yellowish aspect induced by chemical species providing the blue blocking properties.
A specific family of high technology products like Transitions® XTRActive® lenses, which allow activation of the photochromic molecules behind the windshield of a vehicle, present the unique advantage of having a light tint indoor and a strong tint outdoor, leading to enhanced blue light-filtering at all times (Fig. 9 and 10) thanks to specific proprietary photochromic molecules that intrinsically absorb in the blue region of the visible spectrum.
![Overlay of un-activated and activated spectra of Transitions<sup>®</sup> Signature™ grey and brown lenses [A] and Transitions<sup>®</sup> XTRActive<sup>®</sup> grey and brown lenses [B]](http://www.pointsdevue.com/sites/default/files/fig9a.jpg)
A
![Overlay of un-activated and activated spectra of Transitions<sup>®</sup> Signature™ grey and brown lenses [A] and Transitions<sup>®</sup> XTRActive<sup>®</sup> grey and brown lenses [B] 2](http://www.pointsdevue.com/sites/default/files/fig9b.jpg)
B
Fig. 9: Overlay of un-activated and activated spectra of Transitions® Signature™ grey and brown lenses [A] and Transitions® XTRActive® grey and brown lenses [B]

Fig. 10: Blue filtering protection offered by Transitions® lenses at 23°C (ISO 8980-3 calculation 380nm-460 nm range)
Visible light reaching the retina is essential for visual perception. Despite several self-protection mechanisms, the retina in the human eye can be exposed to light levels that exceed its natural defenses and can cause long-term irreversible damage. The lifelong buildup of light-induced phototoxicity can contribute to age-related changes and retinal cell degeneration.
Preventing excess exposure and accumulation of blue-violet light indoors – and especially outdoors – during one’s life seems like common sense.
Transitions® photochromic lenses – and, in particular, Transitions® XTRActive® lenses – offer the optimum visual experience, regardless of lighting conditions, while providing an ideal protection against blue-violet light under all circumstances (Fig. 11).

Fig. 11: Blue light benefits delivered by different optical solutions in the eyewear industry
Article trouvé sur : www.pointsdevue.com
Article trouvé sur : Points de Vue Nr. 72
Source : magazine Points de Vue








Reference : Sheedy, J., Visual fatigue, Points de Vue, International Review of Ophthalmic Optics, N70
Many of our patients have symptoms of discomfort associated with performing near tasks. Of course, the most common tasks performed at near involve reading – especially at computer displays [1] . Therefore it becomes the task of the practitioner to diagnose the conditions causing the symptoms and to devise a treatment plan to eliminate or at least mitigate the symptoms.
The reading task itself, whether on hard copy or electronic display, is perhaps the most visually-demanding near task. Typical reading involves a series of 200 ms fixations sandwiched between 35 ms saccades – each saccade moves the eyes 7-9 characters further in the text. Although this is very demanding, we have discovered that it is the cognitive uptake system that limits reading speed in subjects with vision systems that are performing well – not the visual system. By manipulating the text size and legibility we have noted that fixation durations and frequency are altered, but the reading speed is maintained [2, 3, 4, 5] . Actually, it is remarkable that many people can read for hours with no symptoms.
Given that reading (near work) can be performed without symptoms under good conditions, it becomes our task to identify the reason(s) why our particular patient has symptoms of discomfort. I have observed clinically [6] and in laboratory research [7, 8,9] that symptoms may occur when either the environmental conditions or the visual system capabilities are compromised. Resolving the patient symptoms often requires analyzing both the visual system and the environmental conditions under which they have the symptoms of discomfort [10].
Analysis begins with scrutiny of the patient symptoms. This can often directly lead the clinician to the correct diagnosis. The symptoms can be categorized into visual, musculoskeletal, and asthenopia as shown in Table 1.

Tab. 1: Three primary symptom categories.
Visual symptoms are the easiest to diagnose. They can easily result from an uncorrected refractive error – errors as low as 0.50 DC can result in symptoms.
Presbyopic patients should be properly corrected for the unique viewing distance of their computer, and will report blur or musculoskeletal ache if not. Typically presbyopic patients require an intermediate prescription in order to see their computer correctly. It is important to determine the distance at which they view their work (office computer displays are typically at a viewing distance of 50-60 cm). Demonstration and refinement of the near addition in free space can reassure both clinician and patient.
Slowness in focusing, or distance blur after near work, is typically due to accommodative infacility. If so, tests of accommodative function can assess if this is a problem. It is best to test accommodative infacility directly using +/- lens flippers.
Double vision (diplopia) is infrequently reported, but indicates a binocular vision difficulty when present. An intermittent diplopia usually indicates an intermittent strabismus. Analyze the binocular vision system to determine if there is an eso or exo strain on the visual system. The most common problem is a convergence insufficiency that causes intermittent exotropia at near distances.
Musculoskeletal sysmptoms
Neck ache and back ache are quite common in computer-using patients. This can often be due to inappropriate location of the display or inappropriate spectacle correction of presbyopia.
The top of the display should be near eye level. If not, then adjustments need made to accomplish this. Our visual system has a strong preference for looking down about 10 degrees – i.e. depressing the eyes about 10 degrees [11]. If the display center is not about 10 degrees below the eyes, then neck and back adjustments are made [12] resulting in strain.
Neck and backache can also be caused by presbyopia-correcting spectacles that cause an awkward viewing distance or posture to see the computer display or other uniquely-located near work. It is very common for general-issue bifocals or progressive addition lenses (even though they might work for most other everyday tasks) to be guilty of this.
Wrist, back, and shoulder pain or ache can also be caused by other work-related factors and referral to a workplace specialist is indicated.
Asthenopia is a catch-all for the less-specific symptoms such as eyestrain.
Our research has repeatedly shown [13–14] that these symptoms fall into 2 constellations both subjectively (i.e. patient sensations) and objectively (i.e. the inducing condition). We call these 2 constellations “external symptoms” and “internal symptoms”. They are summarized in Table 2.

Tab. 2: External and internal symptoms
In general, the differentiation can be summarized as follows:External and internal symptoms
The clinician can use this symptom differentiation to help guide the diagnosis and management of the patient. External symptoms indicate a dry eye condition and possible environmental culprits such as lighting, display location, or text quality. Internal symptoms indicate an ophthalmic or visual problem related to accommodation, convergence, or refractive error. Clinicians may want to use the clinical tests shown in Table 3 to diagnose accommodative and binocular vision disorders.

Tab. 3: Tests for accomodation and binocular alignment
After diagnosing the reasons, either environmental or visual, that cause or contribute to the symptoms of discomfort, then the appropriate treatment measures from those below can be used to treat the patient.
To begin, the location of the primary work (e.g. computer display) must be determined. If a computer display location can be altered, then it should be located so that the top of the display is level with the eyes. If the display cannot be located differently, then its location should be noted and spectacles designed accordingly.
Most younger presbyopes (near add of 1.25 D or less) can often use their regular bifocals or PAL for their intermediate work (e.g. computer display). This is because such patients have enough remaining accommodation that they are able to comfortably view and focus upon the intermediate task through the distant portion of their spectacle lenses.
Presbyopic patients with a near add of 1.50 D or greater often require separate spectacles for performing near work comfortably if that near work is at a unique viewing angle or distance, such as commonly occurs at computers or on assembly lines. If the patient wears bifocals for everyday needs, then it is likely best to provide the patient with work-related bifocals in which the top contains the intermediate prescription and the bottom contains the near prescription. Trifocals may be considered. If the patient wears PALs for everyday viewing, then it is best to provide Occupational Progressive Lenses (OPL) for the patient. OPLs are designed to provide extensive intermediate and near viewing areas. Usually the top of the lens also contains a small add of +0.50-0.75D. OPLs are very useful for most office and other indoor activities.
In prescribing adds and designing spectacles, it can be very useful to demonstrate the add and clear viewing distances in free space. If prescribing an OPL, it is also very useful to demonstrate the small distance blur through the top of the OPL so that there are no surprises at time of dispensing.
Dry eye is a common complaint among office and computer workers. Very often the following conditions contribute to dry eyes and fixing them can improve the symptoms:
In addition to the above measures, it is advisable to provide artificial tears to be used only as needed. Counseling about work breaks and light rubbing of the lids may also be helpful. More severe cases of dry eye require additional measures such as punctual plugs.
Reduced amplitude of accommodation (for the patient’s age) and accommodative infacility can both be managed with either orthoptic training or prescription of plus lenses (usually +0.50 to 1.00D) for near work. Working patients often are unwilling to spend the time with an orthoptic program, and the plus lenses can cure the problem.
Likewise, patients with esophoria at near are best treated with a near add, which reduces the eso stress on their binocular system.
Patients with exo deviation, as often accompanied by convergence insufficiency, must be treated with orthoptics – lenses are not an effective treatment. Fortunately, convergence is the most easily trained visual function and can often be managed with push-up training alone.
Lighting is likely the most common environmental culprit insofar as causing and contributing to visual discomfort. All patients with near viewing symptoms should be counseled about eliminating glare from lights.

The most common lighting problem is shown in the picture above: light from luminaires (or windows) directly impinging the eyes of the patient – i.e. the light source is very bright in the peripheral field of the patient. This can be demonstrated to the patient by taking the patient to an office location with a bright overhead light, and requesting the patient to shield their eyes from the offending light with their hand. Patients should be encouraged to note the improved comfort by doing so. The patient can then be instructed to repeat the test at their work place to test if lighting is a problem.
If lighting is determined to be a problem, then possible interventions include: turning off the offending light, use blinds or drapes on windows, remove white surfaces, use partitions, rotate the work station, use indirect lighting, or wear a visor.
For visual and musculoskeletal comfort, the work to be viewed most often must be directly in front of the person and located so that the person views it with eyes depressed at least 10 degrees and no more than 30 degrees. For computer displays, intended to be used with an upright posture, the top of the display should be at eye level, resulting in eye depression to view all elements of the display.
Upright posture while maintaining the normal convex curvature of the lower spine can be important to long term comfort. Arms should be supported by chair arm rests to avoid tension across the shoulders. Variable positioning, such as adjustable height desks and chair also can improve patient comfort.
Reference : Sheedy, J., Visual fatigue, Points de Vue, International Review of Ophthalmic Optics, N70
Source : www.pointsdevue.com









